SCAGO

Table of contents
The study was carried out by Sickle Cell Awareness Group of Ontario formerly known as Seed of life Philanthropic Organization Between August 2005 and March 2007.
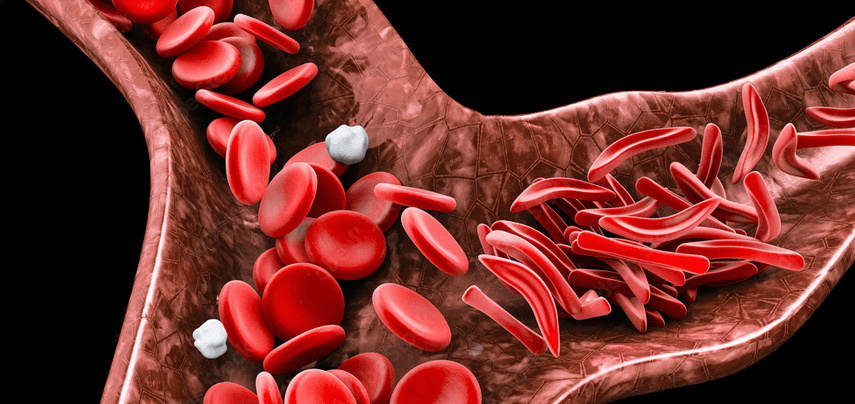
What is Sickle Cell Disease (SCD): It is a genetic blood disorder that affects the red blood cells. It causes the red blood cells to become hard and sickle-shaped which makes it difficult for the blood cells to travel through the small blood vessels. Normal red blood cells are round and last approximately 120 days while the red blood cells of a sickle cell patient last for only 10-20 days.
Sickle Cell Disease affects those whose ancestors are from Africa, the Caribbean, Latin America, South America, India, Asia, Middle-East& the Mediterranean.
Globally, a quarter of a million children are born with the disease each year with the majority from Africa.
With the growing number of people of African ancestry migrating and living in Canada, it is of paramount importance to understand how to reach these people along with the other ethnic groups affected by SCD.
Unlike Cancer, SCD has been treated as a minority problem. This has hampered funding that could have helped to understand why it is rampant within some cultures more than the others even in the at-risk communities and to find ways to support those living with the disease.
Very little study has been conducted if any at all on understanding these grassroots cultures.
We found that many Africans for instance, are coming from cultures where any incidence perceived negative is considered shameful by the family and to avoid shame, many will hide the perceived negative event/occurrence. For instance, for many years it was believed that a marriage producing only female children is negative and the fault is the women. Many times, such a woman would be sent packing simply for not being able to produce a male child.
Similarly, losing one’s child while one is still alive is considered a curse by the gods.
It is not surprising then to realize that having a disease such as sickle cell is unacceptable and considered shameful.
Hence, many families refused to discuss their children’s health deficiencies even with their extended family members and neighbors. This is for the fear that the children will be labeled as “soon to die” and everybody will look down at their family as “the family with the sick child”
With no support group to help and no one that understands the stress, many carry the burdens of raising sickly child/children alone.
This is the culture that many immigrants in Canada are coming from.
To be able to reach both the young and the old from these cultures, we must understand who they are, their beliefs and it is only then that we will be able to let them know that there is no shame in having SCD while educating them on the choices available to them in order to prevent more incidences of the disease.
It is important to let individuals from ethnic cultures with a high incidence of this disease understand that having genotype testing (Hemoglobin Electrophoresis) is a good way to know their sickle cell status. It will help to eliminate the ignorance and secrecy that surround this disease. Many will be more open and discussing sickle cell disease will no longer be such a taboo.
Doctors, nurses, social workers, caregivers, counselors need to understand what the challenges of the people from different ethnic groups are and hear about their experiences & thoughts in order to be able to provide care that targets total needs.
In Mid-2005, the Sickle Cell Awareness Group of Ontario (SCAGO) started to actively visit churches and other venues where ethnic groups, both young and old are; in other to educate them on sickle cell disease.
Various interactive forums & interviews were conducted and questionnaires were given out to be filled.
From many of the responses, it was realized that many of the at-risk communities are not well understood by both the medical practitioners and the extended community.
SCAGO realized that it must work with the community leaders, medical and allied health practitioners, and spiritual leaders if many in the At-Risk communities must be reached, educated, and supported.
A few of the leaders that we are currently working with are:
Spiritual & Community Leaders:
Rev. Audley James-Founder and Senior Pastor, Revival Time Tabernacle Senior
Apostle Igberase- Senior Pastor, Christ Chosen Church of God Pastor
Tayo Ojajuni- Senior Pastor, the Redeemed Church of God
Mr. Lawson- President, Nigerian Canadian Mosque.
Medical Professionals:
Dr. Isaac Odame – Hematologist, Hospital for Sick Kids
Dr. Olaniyi Ajisafe – Family Physician, Safe Care Medical Center
August 2005-March 2007: Questionnaires were given out at different events and churches. Over 350 questionnaires are used for the purpose of this study, subjects’ ages ranged from 18 to 75. This group includes youths, parents, and grandparents. Including their names are optional. Out of 350 questionnaires sampled, 200 have heard about SCD and genotype testing at one time or the other.
150 have heard about SCD but hearing about genotype testing for the first time
Out of the 200 people that knew about genotype testing, 105 know their genotype from their country while 95 have not been tested. These indicated that they will go for this testing at a later date due to the impact of the seminar/forum.
Out of the 150 that are hearing about genotype testing for the first time, 120 decided that they will go for this testing while about 30 are indifferent.
The locations/events where the questionnaire samples are collected
Christ Chosen Church ofGod,
The Redeemed Christian Church ofGod,
The Nigerian CanadianMosque,
Planet Africa Television’s 2006 Forum on Sickle cell anemia,
Malvern ChristianAssembly,
SCAGO’s May 27th, 2006 Forum on Sickle Cell Disease & other communal Issues.
Questions asked were meant to show attitude towards SCD, the familiarity of subjects with genotype testing if they have had it done, and if not, has the seminar/event they are attending influenced them to want to get this testing done for both themselves and their children.
SafeCare Medical:
SafeCare Medical included a hemoglobin electrophoresis test in the blood work of all patients for a period of three to six months. The test results identified 1 in 4 of individuals from specific African cultures as carriers of the sickle cell trait. Nigerians ranked highest on the list of carriers.
About this booklet
This booklet provides an overview of the questions asked in the questionnaire and the interview conducted with comments from individuals living with SCD, mothers living with sickle cell patients, youths who do not know their carrier status, carriers of the sickle cell genes, a family doctor as well as community and spiritual leaders from the At-Risk Communities of Jane/Finch and Scarborough areas.
We hope that reading this study will:
Help both parents and young people, especially from the African cultures where there is a strong shame stigma attached to this disease, that there is really no shame in having SCD or carrying the
Help the health care professionals understand the needs of the different cultures represented in Canada as evident in what some considered shameful and hopefully help them overcome the unnecessary stigma while recommending adequate testing and care that will improve their state of
Help many patients and their family members become more open and join various support
Encourage many to get the Hemoglobin Electrophoresis testing
Help turn SCD from a hush disease to an openly discussed
Reduce the level of ignorance and stigma associated with SACD
Help many immigrants from the At-Risk communities understand the culture of their new country and the need to freely adapt and assimilate the openness of Canadian Culture, especially where it comes to discussing
Our contact information is at the back and we hope that as many as needed genetic counseling and more information about sickle cell disease will feel free to contact us whenever they wish.
Talking about Sickle Cell Disease (SCD) and Genotype testing
Many in the African and the Caribbean communities who have children or siblings living or dead from the complications of SCD do not want to talk about this disease, hence the necessity for us to let them know that they do not have to fill in their names on the questionnaires and for the interviewees, their names would not be mentioned as well. “There is a feeling of shame and it is looked at as a taboo within the community. It just makes others think that something is definitely wrong with your family and who will marry from a family that has such an incurable disorder.
It is best to be left as a secret. It is not a nice thing”. Said one of the African ladies interviewed
Some patients believed that to find a partner to marry them, they have to hide this condition.
Some of the participants that we interviewed believed that this secrecy stemmed from a culture whereby the less fortunate and the handicapped are looked down at. You have to be normal in every aspect to be accepted.
A lady said “When I arrived from Ghana, about 15 years ago, I was shocked to watch a lady come on live television and talked about how she had cancer”
We will never talk about things like that! We need a lot of help in adapting to the culture of speaking about our problems and issues”
Another concern for many also is the fact that they felt that many Canadian doctors neither understand the disease nor the emotional stress suffered by those affected by it and their families.
A 35-year-old patient said “I was rejected by many doctors on arrival from Nigeria, about three years ago. They kept telling me that I should find another doctor as they do not understand my disease. I eventually have to look for a doctor whose background is African”
She also mentioned that the ER medical professionals need to understand SCD more. On one of her emergency visits, she was left at the ER in excruciating pain for over 8 hours before finally being attended to. She added that a nurse told her that the reason she visits the hospital so often is that she is an addict who is now addicted to the medications. This shows the level of ignorance about sickle cell and the excruciating pain associated with it even among the medical professionals” she said.
It is our hope that this study will help both caregivers and the medical professionals understand that it is not that the SCD patients wanted a fix as they are not drug addicts but are living with a disease that affects minority groups and need to be understood properly if adequate help will be rendered to them.
Some of the young people who completed the questionnaires and were also interviewed whose age range between 18-35 unbelievably do not know their genotype even though many of them have seen some individuals go through the painful crisis associated with this disease.
Most of them believe that it is important to know one’s genotype but has not gotten around to it, while others don’t seem to think too much about it.
A young man said
“I am healthy and rarely fall sick, why should I worry about genotype testing?”
Another said “If you are man enough, you will not have children with SCD”
These responses clearly showed a lack of adequate education and knowledge on this matter.
Racial Discrimination
Most of the participants being interviewed believed that provinces such as Ontario which is home to many diverse minority groups that are affected by (SCD) are not doing enough to reduce the incidence of this disease. They suggested that the Ontario government should stop seeing it as a minority issue but as an Ontario problem, after all, more sickle cell births mean more money spent by the Ministry of Health on patient care.
Why not direct some resources to research, education, and support for the at-risk communities.
“We are part of this system and our issue should not be seen as just a minority issue,” said an elderly interviewee.
Asking those who know—-
Speaking to those who are suffering from SCD and those who have lost close relatives to this disease, the overall important perspective on this disease and —-
What they will like to see includes the following:
“Educating our young people to know their carrier status when it comes to genetic disorders such as SCD is important if we want to reduce the number of children being born with this disease”.
“Children born with SCD should be born out of parental choice and not ignorance”.
“African-Canadians and other groups should be reached more readily when it comes to genetic counseling.”
“Medical professionals, nurses, and other caregivers should receive ongoing training about this disease and how to deal with sufferers”.
“Every Ontario doctor should not turn patients away but strive to understand the disease”.
“More Organizations educating people on this disease should be adequately funded”.
“There should be a resource center or some sort of special counseling center for communities such as African & Indians whose background cultures and attitude towards many issues are different from the Canadian culture”.
“Maybe there should be a group for spouses of those living with SCD” “
Those with SCD should be supported more as many of us are highly educated with university degrees but could not hold jobs because of the frequent in/out hospital admission” said a patient.
Comments:
Seed of life works to educate and inform the minority at-risk groups on SCD and how their future generations could avoid the agony of a disease that comes with complications such as acute chest syndrome, damage to the vital organs of the body including the heart, liver, kidney and the spleen. It also causes diabetes, high blood pressure, blindness, stroke, and premature death.
SCD comes in different forms chiefly among which are Sickle Hemoglobin C (SC), Sickle Cell Anemia (SS), Sickle Beta-Plus Thalassemia, and Sickle Beta Zero Thalassemia.
It affects people from the Sri-Lankan, Indian, Latin America, South America, Middle East, Caribbean, Asian, the Mediterranean as well as the African communities.
Many are dying from its complications while more parents and caregivers are stressed as they helplessly watch their loved ones suffer from the pain & agony of this disease. Thus many wish that the doctors and caregivers understand this disease more.
Seed of Life is working hard to reach at-risk groups affected by the different types of SCD with its educational campaign.
Articles